Reacting to Zika Without Overreacting
Zika virus (ZIKV) is in the news, and the volume is deafening. Florida Governor Rick Scott declared a health emergency in that state after nine cases were detected in four counties. The World Health Organization (WHO) declared Zika an international health emergency. A recent headline from the Times of India claims, “Alert Sounded Over Deadly Zika Virus in Gujarat.” It sounds serious, but as far as we know, Zika is not deadly, and there hasn’t even been a single reported case in India. Is Zika really an international health emergency? What is causing this panic, and what should be our focus? To evaluate realistically the impact of this virus and develop control strategies, let’s review what is known, understand the real transmission risk, and look at how we have managed similar outbreaks in the past
What We Know About ZIKV
Illustration of the Zika virus
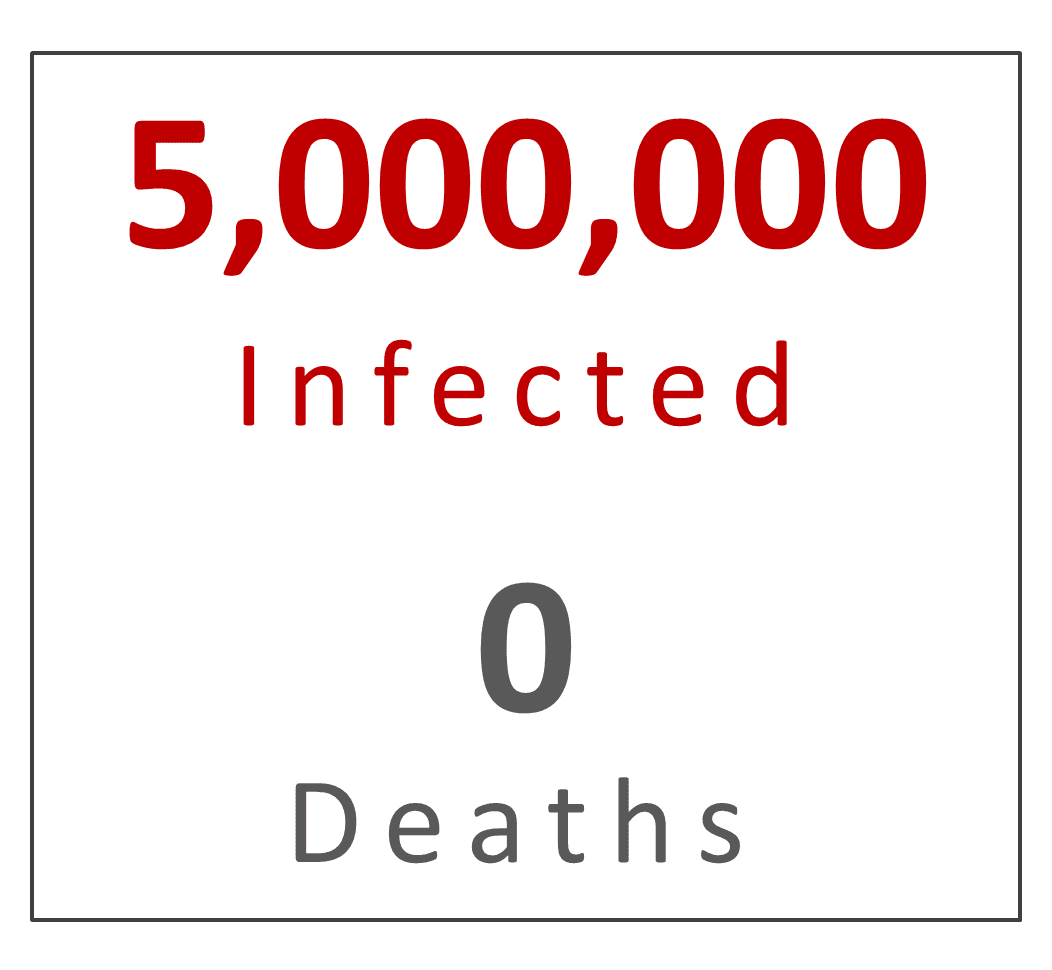
Infection with ZIKV causes fever, rash, headaches, conjunctivitis, and joint pain. According to the Centers for Disease Control and Prevention (CDC), about one in five people (20%) infected with ZIKV will show these symptoms. ZIKV is not a new virus. It was discovered in Uganda in 1947 and has since been detected in tropical Africa, Southeast Asia, and the Pacific Islands. ZIKV was recorded in the Western Hemisphere first in 2014, and ZIKV transmission in Brazil was reported by the Pan American Health Organization (PAHO) in May 2015. To date, reports of 500,000 to one million clinical cases of ZIKV infection have been reported in Brazil. Because only 20% of infections manifest clinically with fever, rash, and joint pain, this means there could have been up to five million people infected (80%, or four million, showed no symptoms). And out of those five million infections, not a single death has been reported.
 Epidemiological data from Brazil indicates an overlap between ZIKV infections and an almost 20X increase in suspected cases of microcephaly, a condition where babies are born with abnormally small heads and brain damage. But according to the Health Ministry of Brazil, only six of the suspected cases of microcephaly are related to ZIKV. Out of one million clinical cases, the 4000 cases of microcephaly equate to an incidence rate of 0.004. In other words, if the virus causes birth defects, 0.4% of clinical cases could result in babies born with microcephaly. This calculation ignores how many of those clinical cases were women of child-bearing age and how many women (uninfected and infected, symptomatic and asymptomatic) gave birth in Brazil in 2015. While a 20X increase in reported cases sounds terrible, most people don’t know that the Brazilian government urged pediatricians and clinics in 2015 to report suspected cases of microcephaly. The New York Times reported that out of 700 suspected microcephaly cases in Brazil, ZIKV was detected in only six infants. Because the baseline numbers for microcephaly are difficult to verify, and there is a risk of overdiagnosis, the correlation between ZIKV and microcephaly is inconclusive. The CDC has stated that it is not certain that Zika causes birth defects, and so it recommends pregnant women avoid traveling to areas of active ZIKV transmission until more is known about the risks.Because Zika manifests as a mild febrile disease with complete recovery, and the definitive cause/effect of ZIKV on the fetus is currently uncertain, claiming ZIKV is “deadly” is irresponsible and unhelpful at this time.
Epidemiological data from Brazil indicates an overlap between ZIKV infections and an almost 20X increase in suspected cases of microcephaly, a condition where babies are born with abnormally small heads and brain damage. But according to the Health Ministry of Brazil, only six of the suspected cases of microcephaly are related to ZIKV. Out of one million clinical cases, the 4000 cases of microcephaly equate to an incidence rate of 0.004. In other words, if the virus causes birth defects, 0.4% of clinical cases could result in babies born with microcephaly. This calculation ignores how many of those clinical cases were women of child-bearing age and how many women (uninfected and infected, symptomatic and asymptomatic) gave birth in Brazil in 2015. While a 20X increase in reported cases sounds terrible, most people don’t know that the Brazilian government urged pediatricians and clinics in 2015 to report suspected cases of microcephaly. The New York Times reported that out of 700 suspected microcephaly cases in Brazil, ZIKV was detected in only six infants. Because the baseline numbers for microcephaly are difficult to verify, and there is a risk of overdiagnosis, the correlation between ZIKV and microcephaly is inconclusive. The CDC has stated that it is not certain that Zika causes birth defects, and so it recommends pregnant women avoid traveling to areas of active ZIKV transmission until more is known about the risks.Because Zika manifests as a mild febrile disease with complete recovery, and the definitive cause/effect of ZIKV on the fetus is currently uncertain, claiming ZIKV is “deadly” is irresponsible and unhelpful at this time.
How Zika is Spreading
ZIKV is transmitted from person to person by the bite of an infected mosquito, Aedes aegypti. Laboratory trials have shown that Aedes albopictus is a competent vector, but we have no evidence of transmission in the field. Right now, we don’t know which other North American mosquito species might be competent vectors of ZIKV, and even A. albopictus in the U.S. would have to be evaluated before it is definitively incriminated. Seasonal and geographic overlap with human cases, host-feeding behavior, field isolations of the virus, and laboratory demonstration of vector competence are necessary to incriminate a mosquito as a vector.Non-human primates are reservoirs for Zika in Africa, but they are not abundant in the U.S. We also don’t know if local rodents or birds can act as reservoirs for ZIKV.

Lastly, it is true that we still don’t understand the role and impact that sexual transmission might have in the spread of this virus. The first documented case of sexual transmission of ZIKV was between a medical entomologist and his wife in 2009. Four years later, during an outbreak in Tahiti, ZIKV was isolated from the semen of an infected man. This week, the first diagnosis of sexually transmitted ZIKV in the U.S. was made in Texas. And because one consequence of unprotected intercourse is pregnancy, sexual transmission could result in ZIKV infection at conception. However, the role of sexual transmission in the spread of ZIKV and the potential of that transmission to cause birth defects are still unknown.
Comparing Zika to Dengue
Dengue is a flavivirus, like ZIKV, that causes fever and joint pain with high rates of asymptomatic infection and is transmitted by Aedes mosquitoes in a human-mosquito-human cycle.Dengue is the most common mosquito-borne viral disease in the world, causing 50-100 million infections and at least 25,000 deaths each year. There were 93 locally-acquired cases of dengue in residents of Hawaii in 2015. In the first six months of 2015, 746,000 cases of dengue fever and 229 deaths were reported in Brazil. To date, 31 cases of ZIKV have been diagnosed in the U.S., all of which were acquired from travelers overseas. Infections acquired overseas are sure to increase, especially after Rio Carnival in February and the Rio Olympics in August. In regions of the U.S. where A. aegypti and A. albopictus are common, these two species will likely transmit ZIKV locally. A vaccine against ZIKV will be years away, assuming there is a market for it, and there are no specific treatments for the symptoms. As with other mosquito-borne viruses, the best method to limit the spread of ZIKV is vector control.
Vector control: Lessons from dengue
Using a systematic approach with mosquitocides formulated specifically for public health is our most immediate and effective weapon against the spread of ZIKV. We know that A. aegypti is the most likely vector of ZIKV, and A. albopictus could also be important. Because these species tend to be urban and suburban, we must focus on strategies that control container-breeding mosquitoes. This means we must implement:
- Surveillance. Use ovitraps/gravid traps to provide samples for virus isolation.
- Source Reduction. Reduce oviposition sites and larval habitats in domestic and peridomestic sites.
- Larvicide Treatments. Treat larval habitats, including obvious sources and cryptic sites, with larvicides.
- Adulticides. Use targeted treatments in response to surveillance triggers.
Surveillance is the first step in an epidemiological response. While the triggers of action vary by region, the general indicators that trigger adulticide spraying include:
-
- Virus isolation from field-collected mosquitoes.
- Clinical diagnosis in a human.
Each of these triggers can be acted upon singly, in parallel, or in a series. For example, isolation of ZIKV from mosquitoes or a human case overrides an increase in mosquito numbers in light traps.



